



 rojectiles. The most imminent danger for both patients and personnel in the magnetic field of an imaging system may result from ferromagnetic objects such as scalpels, scissors, pens, and even sand bags (not filled with sand but with iron shot) and gas dewars, which can be attracted by the magnet and thus behave like projectiles.
rojectiles. The most imminent danger for both patients and personnel in the magnetic field of an imaging system may result from ferromagnetic objects such as scalpels, scissors, pens, and even sand bags (not filled with sand but with iron shot) and gas dewars, which can be attracted by the magnet and thus behave like projectiles.
To prevent such accidents, the installation of a metal detector through which everybody has to pass before entering the MR suite has been recommended, but is rather cumbersome. Instead, automatically locking doors with badge access are recommended.
 Monitors and respirators. The dependence on physiological monitoring, on mechanical respiration, and electric infusion pumps during MR examinations renders difficulties, and in certain instances does not allow such an examination.
Monitors and respirators. The dependence on physiological monitoring, on mechanical respiration, and electric infusion pumps during MR examinations renders difficulties, and in certain instances does not allow such an examination.
However, with the development of appropriate monitoring and life-support equipment during the last few years, dependence is no longer a contraindication of MR imaging. Details on monitoring can be found, for instance, in an official Canadian publication [⇒ Medical Advisory Secretariat 2003].
Contrast agents. Magnetic resonance contrast agents or other substances which have to be injected or applied in another way may present risks similar to those in any other invasive technique such as x-rays, particularly in patients with kidney diseases. In patients with kidney diseases certain contrast agents are contraindicated and were removed from the market in a number of countries (cf. Chapter 13. Adverse Events).
The clinical experience of administering gadolinium-based or other agents intravenously to patients has shown that these agents are generally safe and well tolerated. Still, all necessary precautions for intensive-care treatment have to be considered when injecting such contrast agents, particularly in patients with a history of allergy and drug reactions. When contrast agents are used according to the given guidelines and regulations such side effects are extremely unlikely.
Field Strength and Hazards. Many of the incidental hazards increase with field strength and the existing research on safety cannot straightforwardly be extrapolated to field strengths beyond 1.5 Tesla. Further studies are required to confirm the hazard-free use of MR imaging at ultrahigh fields. Until proven otherwise, patient studies at ultrahigh fields should be considered carefully.
Noise. The noise created by the switching of the gradients is an additional source of inconvenience and can cause ear damage to the patient and, occasionally, personnel [⇒ Radomskij 2002].
Sound pressure levels (SPL) increase with field strength. The noise levels at 3 Tesla can approach twice those of those at 1.5 Tesla. Sound pressure levels at the center of a head coil can exceed 130 dB(A). British and US American guidelines stipulate that the maximum permitted daily noise dosage is equivalent to 90 dB(A) for 8 hours; the guidelines for Europe allow only 80 dB(A) for 8 hours [⇒ Foster 2000].
Noise-canceling systems and special earphones are available, and active acoustic control systems are being developed [⇒ Mansfield 1981]. At fields of 1.5 Tesla earplugs and headphones are strongly recommended; at higher fields they are mandatory. Even with hearing protection there can be hearing loss after examinations at 3 T [⇒ Jin 2017].
Acoustic noise can cause detrimental effect in both term and preterm neonates; they should be examined at field strengths below 1.5 Tesla, if possible in dedicated equipment [⇒ Tkach 2014] (cf. Chapter 3).
MR imaging is used for fetography (Figure 18-07), particularly for imaging the brain. At 3.0 Tesla (or higher magnetic fields), the specific absorption rate (SAR) and the increased noise may, at least potentially, adversely affect the fetus [⇒ Cannie 2016].

Figure 18-07:
MR fetography in the 32nd week of pregnancy.
Cooling gases. In superconductive magnet systems, helium and still occasionally nitrogen are used as cooling gases. In the case of a quench, gases are released to the outside. Under normal circumstances, the gases should escape through a pipe system and not reach the magnet-room atmosphere. However, accidentally some gas could be released into the magnet room.
In this case, there are two potential dangers. Frostbite can be induced because the gases are extremely cold. Secondly, nitrogen is to be considered hazardous, in particular under pressure (whereas there is no danger of direct intoxication from helium).
All personnel and patients must evacuate the area immediately and return only after proper ventilation of the magnet room.
It is beyond the scope of this textbook to provide guidelines for every implanted device. For many implants (e.g., pumps, infusion system, and tissue expanders) manufacturers propose detailed MR procedures. Numerous of these implants are MR unsafe or MR conditional which also means unsafe in daily routine. Devices declared MR Safe for 1.5 Tesla might not necessarily be safe at higher fields.
There are a number of guides covering all different kinds of implants. A general review and explanation of MR labeling information for implants and devices was presented by Shellock and collaborators. They also gave an extensive overview of the behavior of implants. Note that such lists are of only limited use because often it is the interaction between a particular device and a particular MR imaging equipment that can lead to complications [⇒ Shellock 2009, ⇒ Shellock 2004].
For clinical MR examinations MR Conditional devices must be considered unsafe if the contrary has not been proven. Some equipment manufacturers offer an automatic adjustment of imaging procedures for MR Conditional devices.
The rate of increase of the magnetic field within the fringe field is described as the spatial field gradient (SFG or SG) and expressed in Tesla/meter or Gauss/ centimeter. A description is given by the International Electrotechnical Commission or, for instance, in a review by Steckner [⇒ IEC 2016, ⇒ Steckner 2012].
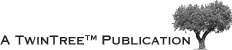
Foreign bodies. Hemostatic or other clips in the CNS can move in their position (Figure 18-08). Dislocation by magnetic attraction or torque presents a risk of hemorrhage. In other parts of the body, we consider this to be a minimal risk, because after the healing phase of six to eight weeks, fibrosis and encasement of the clip help to keep it in a stable position.
Figure 18-08:
X-ray of a head showing clips after a brain operation: safe or unsafe for MR imaging?
Occult ferromagnetic foreign bodies incorporated in accidents are dangerous, in particular those close to the eyes.
The patient's history may help to rule out such foreign bodies. Many patients, however, do not remember such accidents. In case of doubt, x-rays should be taken prior to MR imaging. Ferromagnetic makeup and tattoos cannot only distort MR images, but can be irritated and makeup can even be pulled into the eye by magnetic forces. Makeup should be removed before the examination, if possible. Pharmaceutical products in transdermal skin patches may cause burns due to the absorption of RF energy. Such patches must be removed prior to MR examinations.
IUDs. Most of the commonly used intrauterine contraceptive devices (IUD) do not move under the influence of the magnetic field, do not heat up during sequences usually applied for pelvic imaging, and do not produce major artifacts in vitro or in vivo at medium, high and ultrahigh fields (up to 9.4 Tesla). Thus, patients with either all plastic or copper IUDs can be safely imaged with magnetic resonance [⇒ Mark 1987, ⇒ Gaa 2017].
Joint and limb prostheses. Generally, such prostheses present no risk. However, they can introduce image artifacts. If possible, they should be removed prior to the MR examination.
Pacemakers. For a long time the rapidly growing group of patients with cardiac pacemakers (PMs) and implantable cardioverter defibrillators (ICDs) had only limited access to MR imaging. These devices used to be an absolute contraindication. Meanwhile, this restriction has been relaxed to Potential Contraindication. Still, patients with pacemakers and similar devices require specific care.
Potential complications during MR examinations of PM wearers include adverse effects including tissue heating, unpredictable reed switch behavior and alteration of pacemaker programs, asynchronous pacing, or damage to pacemaker circuitry, and electrode and lead displacement.
The US-American Food and Drug Administration underlines that there are weak points in the studies of MR imaging in patients with pacemakers and implantable cardioverter defibrillators [⇒ Faris 2006]. It seems to be imprudent for patients with certain cardiovascualar devices to undergo MR imaging. Judicious scrutiny with careful patient screening and exact and reliable assessment of the implanted device are compulsary before an MR examination of such a patient.
Monitoring of ECG, blood pressure measurement, and pulse oximetry by trained personnel during the MR study is absolutely necessary. Recommended procedures vary; in some places the presence of an anesthesiologist or cardiologist is standard for the preparation and immediate follow-up of the patient.
The current scientific statement from the US-American Heart Association does not comment on SAR limitations [⇒ Levine 2007]. However, the European Society of Cardiology recommends a SAR limit of 2 W/kg [⇒ Roguin 2008]. It is recommended to adjust the highest possible SAR for each sequence to ≤2.0 W/kg, preferably to ≤1.5 W/kg. Note that the SAR of an identical pulse sequence at 1.5 Tesla quadruples at 3.0 T and is more than twenty times higher at 7.0 T. Therefore, the maximum field strength for studies of such patients is 1.5 T.
Other Implants. Similar considerations hold for pacemakers used for stimulation of the carotid sinus or intracorporal insulin pumps. Here, no adverse effects have been observed [⇒ Schröder 1987]. However, interference in electronic cochlear implants and ferromagnetic mechanical stapedial replacements has been reported [⇒ Hepfner 1985]. Prosthetic heart valves are not considered to be dangerous in low fields [⇒ Soulen 1985]. However, patients should not undergo MR imaging in high or ultrahigh fields if valve dehiscence is clinically suspected.
Implants that involve magnets such as magnetic sphincters, stoma plugs, dental implants, etc., can be demagnetized by the MR equipment. They should be removed prior to the examination.
The label stainless steel is not a guarantee for non-ferromagnetic steel.
Wires, other metallic objects, and skin contact. Wire configurations such as pacemaker lead wires, ECG and plethysmographic cables, and surface-coil connections can act as antennas. Gradient and RF fields may induce current into these wires and thus cause fibrillations and burns (Figure 18-09). This presents a risk to the patient and must be eliminated prior to the examination.

Figure 18-09:
Burn on the back of a patient who underwent MR imaging while lying on an ECG lead.
In a similar way this holds for all clothing containing metallic threads or components, as well as all metallic objects such as eye glasses, jewelry, hairpins, buttons, watches, bracelets, prostheses, etc. All of these objects must be removed prior to the examination.
The patient’s skin should not be in contact with the inner bore of the magnet. Large-radius wire loops should not be formed by leads or wires that are used in the magnet bore. If the patient’s arms and legs are not completely covered with clothing, insulating material must be placed between the legs, and between legs and magnet. Leg-to-leg and leg-to-arm skin contact must be prevented in order to avoid the risk of burning due to the generation of high current loops if the legs or arms are allowed to touch.
Claustrophobia. This is a very real psychological danger for some patients. Claustrophobia and other psychological stress situations have been reported to be severe enough to interrupt the examination in about 1-4% of cases. A high incidence of claustrophobia requires additional psychological training of doctors and staff.
Explanation of the imaging procedure and the equipment prior to the examination helps to reduce claustrophobia significantly. Friendly, compassionate, and caring bedside manners help avoid claustrophobia. The contact, dialog and understanding between patient and radiographer are among the most important ingredients of a successful MRI examination.
According to a Norwegian study most claustrophobic patients are able to complete their examination when some effort is made to support them corresponding to their individual needs [⇒ Landrø Svarliaunet 2014]. The following actions are simple, but very practical and helpful. They indicate a positive attitude towards the patients' problems and aid the patients in building up the confidence in themselves to manage the situation.
The patient should be given:
 general information in advance, including the room, the location of the operators' console, the MR machine and the positioning of the patient;
general information in advance, including the room, the location of the operators' console, the MR machine and the positioning of the patient;
an explanation of the strategy and handling of the examination;
a debriefing.
Concerning the examination itself:
A mirror to the head coil helped a quarter of the patients to feel more comfortable;
whenever possible patients should enter the machine feet first;
an accompanying person, laying a hand on the patient's feet, makes it easier for the patient to cope with the situation;
patients in pain should be comforted with, e.g., an extra cushion or straps, helping them to find a comfortable position that they can keep during the examination;
to shorten the examination time for patients in pain or being extremely uncomfortable inside the magnet, the application of pre-planned "short pulse sequences" for the examinations have proven helpful;
using a coil which might not be the optimal or common for the kind of study but suits the patient;
if possible, allowing certain patients to come out of the magnet between sequences;
(a lot of) "chatting" between the scans.
Which strategy to be used depends on the patient. When given some advice about how to handle stress inside the magnet, most patients achieve the needed feeling of self-control. Communication leads to the choice of the right strategy for the individual patient, as the radiographer can act and adjust the examination on the response of the patient.
Small, open, wide-bore and low-noise MR machines are advantageous because the percentage of claustrophobic incidents drops significantly.
The possibility of the patient falling from the examination couch and hypotonic syndrome (due to heat, motionless horizontal lying for a certain time, and psychological agitation) are additional hazards.
Claustrophobia, MRI and the human factor.
 A little more about this topic …
A little more about this topic …
Pregnancy. There is no evidence that MR can harm the fetus or embryo. An epidemiological study by Kanal et collaborators concluded that data collected from MR imaging technologists were negative with respect to any statistically significant elevations in the rates of spontaneous abortion, infertility, and premature delivery [⇒ Kanal 1993]. As a safety precaution, MR scanning should be avoided in the first three months of pregnancy.
With imaging times shorter than 30 minutes, normal SAR regimens did not lead to temperature increases above 1° C in pregnant animals. However, longer imaging times can lead to an increase of 2.5° C. Therefore some major hospitals refer pregnant women to 1.5-Tesla (or lower field strength) machines.
MR imaging is indicated for use in pregnant women if other non-ionizing forms of diagnostic imaging are inadequate, or if the examination provides important information which would otherwise require exposure to ionizing radiation such as x-ray or CT.
Similar considerations hold for pregnant staff of a magnetic resonance department. Mainly for psychological reasons, it might be a wise precaution that pregnant staff members do not remain in the scan room during actual scanning; however, they are allowed to prepare and position the patient, administer contrast agents, and to scan.
Sedation. MR has become an important tool in pediatric imaging. Since some infants and children are unable to cooperate with the examiners, there is an increased demand for sedation.
Some infants sleep soundly through an MR examination, particularly if they have eaten; however, many infants and children up to eight years require sedation, even if they are accompanied by their parents into the scanner room.
In most instances, teenagers can be treated like adults.
Details on sedation and procedures can be found in the literature [⇒ American Academy of Pediatrics 1992, ⇒ Kanal 1992].



|

|
|---|